
Conditions We Treat \u00b7 Forest Hills, Queens
Crohn’s Disease
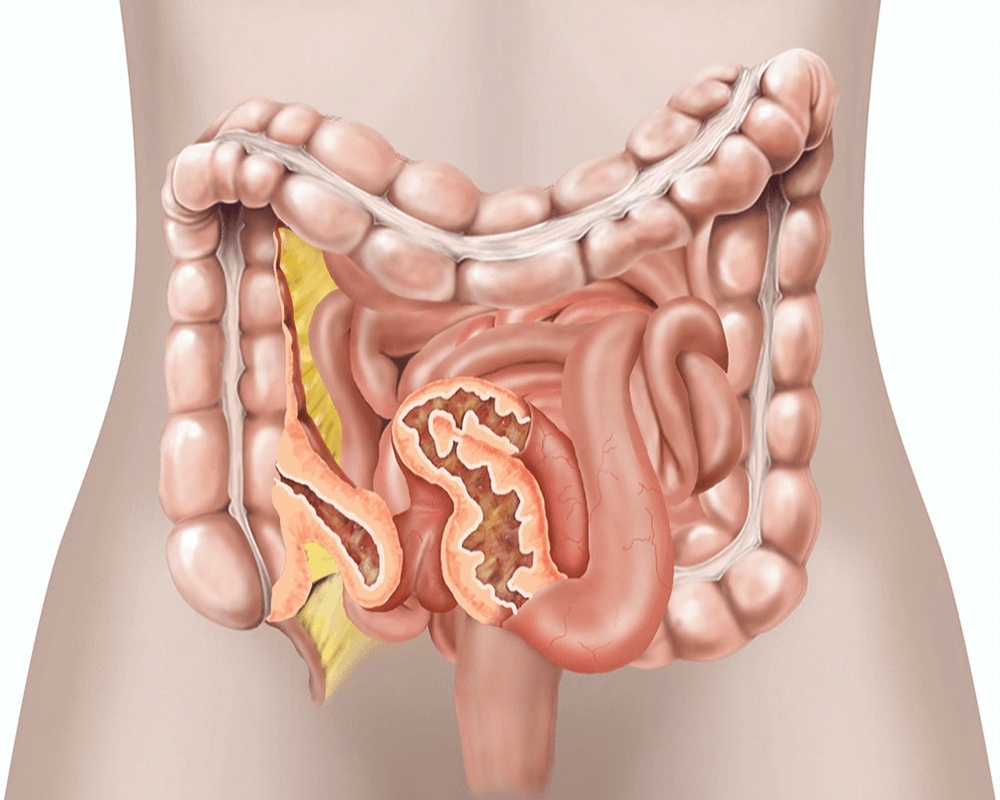
Crohn's disease is a disorder that causes inflammation of the gastrointestinal (GI) tract. The inflammation is usually found in the small intestine (the ileum), but can occur in any area of the GI tract, which stretches from the mouth to the anus. Crohn's is an inflammatory bowel disease, which, like irritable bowel syndrome and ulcerative colitis, causes swelling of the intestines.
(718) 261-0900While IBD may occur at any point in time, it usually appears in patients between the ages of 15 and 30 years old. It has been estimated that more than one million people in the United States are affected with IBD.
Schedule Consultation Check Insurance Medically reviewed by Dr. Samuel Davidoff, MD, Board-Certified Gastroenterologist & Hepatologist | 18+ Years Experience | Last Updated: April 2026
Your Crohn's Disease Specialists in Forest Hills, Queens
Dr. Samuel Davidoff, MD, has treated patients with Crohn’s disease for over 18 years at Gastroenterology and Nutrition, P.C. in Forest Hills, Queens. Board-certified in Gastroenterology and Hepatology, he takes a personalized approach to IBD management, working with each patient to find the treatment combination that achieves and maintains remission.
One of our key diagnostic capabilities is capsule endoscopy. This technology allows Dr. Davidoff to visualize the entire small intestine, areas that standard colonoscopy and upper endoscopy can’t reach. For Crohn’s patients, this matters because the disease frequently involves the small bowel, and identifying inflammation early in these hard-to-reach segments changes treatment decisions.
Dr. Yuriy Israel, MD, board-certified in Gastroenterology and Internal Medicine, works alongside Dr. Davidoff to provide ongoing IBD care. Our AAAASF-accredited procedure suite allows us to perform colonoscopies and other evaluations on-site, in a facility that meets hospital-grade safety standards. Emanuel Yaakobov, FNP-BC, supports continuity of care through regular follow-up and patient coordination.
Types of Crohn's Disease
Ileocolitis
Ileocolitis is the most common type of Crohn's disease, affecting the small intestine (ileum) and the large intestine (colon).
Ileitis
Ileitis differs from ileocolitis in that it only affects the small intestine. In addition to the symptoms of ileocolitis, patients may also suffer fistulas (abnormal tunnels) or inflammatory abscesses.
Jejunoileitis
Jejunoileitis affects the jejunum, the upper half of the small intestine, resulting in cramping after meals, diarrhea, severe abdominal pain and the development of fistulas.
Gastroduodenal Crohn's Disease
Gastroduodenal Crohn's disease affects the stomach and the duodenum. Patients experience more upper digestive symptoms, including nausea, and sometimes, vomiting.
Crohn's (Granulomatous) Colitis
Crohn's colitis affects only the colon. Symptoms include skin lesions and joint pain, as well as diarrhea, rectal bleeding, ulcers, anal abscesses and fistulas.
Causes of Crohn's Disease
The causes of Crohn's disease are not entirely known, but it is believed that people with Crohn's have abnormal immune-system reactions, in which food and bacteria are mistaken for foreign substances. When the immune system tries to attack these substances in the digestive tract, inflammation in the intestines is the result. Crohn's disease may also enter the body as an infection. Risk factors include:
- At Gastroenterology & Nutrition P.C. in Forest Hills, Queens, our board-certified gastroenterologists, Dr. Yuriy Israel and Dr. Samuel Davidoff, provide comprehensive Crohn’s disease management, from diagnosis through long-term treatment. Being younger than 30
- Being Caucasian or of Eastern European Jewish descent
- Having a family history of Crohn’s
- Smoking
- Living in an urban area
Symptoms of Crohn's Disease
The main symptoms of Crohn's disease are diarrhea, which often occurs up to 10 or 20 times a day, and abdominal pain and cramping. Inflammation in the intestines causes an excess of water and salt to be secreted. Because the colon cannot properly absorb the excess, it empties often, resulting in frequent diarrhea. Additional symptoms may include:
Crohn’s disease symptoms may be experienced on a recurring basis, and for irregular lengths of time.
- Bloody stool
- Ulcers
- Reduced appetite
- Weight loss
- Fever and fatigue (in severe cases)

Diagnosis of Crohn's Disease
Blood Test
A blood test is performed to check for anemia, a condition in which there are not enough blood cells to carry oxygen through the body, and which can cause bleeding in the intestines. The blood test also checks for signs of infection.
Flexible Sigmoidoscopy
During a flexible sigmoidoscopy, a slender, flexible, lighted tube is used to examine the sigmoid, which is the last section of the colon.
Colonoscopy
During a colonoscopy, a thin tube with a camera at the top is used to view the entire colon; tissue samples may be taken for a biopsy. Colonoscopy checks for granulomas, clusters of inflammatory cells that, if present, confirm a diagnosis of Crohn's.
Barium Enema
A contrast dye called barium is inserted into the bowel to create a silhouette of the intestines and to highlight any inflammation, which is then viewed through an X-ray. If symptoms of Crohn's disease are present, a medical professional should be consulted. After a thorough physical examination, a series of tests may be performed to confirm the disease's presence. In addition to MRI and CT scans, the following tests may be performed. Colonoscopy is preferred to sigmoidoscopy because it provides a view of the colon in its entirety. Removing tissue to check for cancer is usually only performed on those who have had Crohn's disease for 8 or more years.
Treatment of Crohn's Disease
01. Medication
Anti-inflammatory drugs are often the first treatment prescribed in order to keep symptoms from developing. Corticosteroids may be prescribed for those with more severe symptoms, or for those who do not respond to milder medications. Immune-system modifiers and antibiotics may also be prescribed. Over-the-counter medications that may be helpful include anti-diarrheals, laxatives, nutritional supplements and pain relievers.
02. Diet and Lifestyle Changes
Awareness of the diet and a focus on nutrition may help to reduce the symptoms of Crohn's disease by restoring nutrients that have been lost, and by encouraging the healing process. Restricting dairy products, and foods high in fiber and fat, may help to prevent flareups of the disease. Quitting smoking and reducing stress are also helpful.
03. Surgery
If drug therapy or other treatments cannot control the symptoms of Crohn's disease, a bowel resection may be recommended to remove the portion of the digestive tract that is damaged. Although surgery can provide a period of remission from Crohn's disease, it frequently recurs. Once Crohn's disease is diagnosed, a treatment regimen, which will depend on the type and severity of the symptoms, is prescribed. Crohn's disease cannot be cured, but it can be treated effectively, minimizing the effect on patients' lives. There are a number of effective treatments. Although Crohn's disease can be debilitating, there are instances in which a person who has the disease is asymptomatic. In those instances, no treatment is necessary.
When to See a Doctor
Crohn’s disease is easier to manage when caught early, before complications develop. See a gastroenterologist if you experience:
- Persistent diarrhea lasting more than four weeks
- Abdominal pain with weight loss you can’t explain
- Blood in your stool
- Recurring fevers without an obvious cause
- Perianal pain, drainage, or recurring abscesses
- Fatigue combined with any of the above symptoms
If you have a family history of inflammatory bowel disease, your threshold for seeking evaluation should be lower. Early diagnosis allows for earlier treatment, which improves long-term outcomes and reduces the risk of complications like strictures and fistulas. Call Gastroenterology and Nutrition, P.C. at (718) 261-0900.
FAQ
Common Questions About Crohn's Disease
Gastroenterology & Nutrition, P.C. · Forest Hills, Queens
Ready to Schedule Your Appointment?
Same-week consultations. Sunday procedures offered. Most major insurance accepted.